
Všeobecné
Cystická fibróza (angl. Cystic fibrosis - CF) je dedičné (genetické) ochorenie s výskytom 1: 3000 živo narodených detí, ktoré sa prejavuje chronickým poškodením dýchacích ciest a pľúc, nedostatočnou sekréciou slinivky brušnej, vysokým obsahom solí v pote a sterilitou u 98% mužov. Podstatou ochorenia je zmena fyzikálno-chemických vlastností hlienu na povrchu slizníc. Hustý hlien narúša normálnu funkciu orgánu a je príčinou väčšiny klinických príznakov.
Diagnostika
Diagnostika sa urobí realizáciou genetického testovania na základe podozrenia pre časté infekcie dýchacích ciest a prítomnosti tráviacich ťažkostí. Genetická diagnostika nie je jednoduchá. Predpokladá sa asi 1800 mutácií, ktoré môžu spôsobiť CF. Na Slovensku sa robí diagnostika 30 najčastejších mutácii a tým sa zachytí 85% ochorení. Od roku 2009 sa u každého novorodenca robí skríningové vyšetrenie na CF. Diagnostika už v novorodeneckom veku je veľmi dôležitá, pretože napriek tomu, že novorodenec ešte nemá veľa príznakov a ťažkostí, včasná starostlivosť a preventívna terapia zlepšuje prognózu, predlžuje a uľahčuje život týmto deťom.
Liečba
Prevencia minimalizuje progresiu ochorenia, preto je dôležité predchádzať nebezpečným nákazam a rizikám prenosu baktérii a to dodržiavaním odporúčaného hygienického štandardu pacientmi, dodržiavaním hygienicko-epidemiologických opatrení v zdravotníckych zariadeniach a účinnou prevenciou je aj očkovanie (napr. bežné očkovania u detí, hepatitída, vírus chrípky, Haemophillus influenze, Streptococcus pneumoniae, v štádiu skúšania je vakcína proti Pseudomonas a.
Rehabilitácia je jedným z prvých krokov liečby a delí sa na techniky uľahčujúce očisťovanie bronchov a na kondičné cvičenia. Odstraňovaním hnisavého sekrétu z dýchacích ciest sa znižuje bronchiálna obštrukcia, odpor dýchacích ciest, zlepšujú sa funkčné parametre a odstraňuje živná pôda pre baktérie. Na podporu tejto techniky možno použiť jednoduché pomôcky ako sú Flutter, R-C Cornet, Acapella, PEP maska alebo technicky náročnejší prístroj The Vest. Vhodným kondičným cvičením sa zvyšuje kardiorespiračná kondícia, odolnosť dychových svalov, zníženie pocitu dychovej nedostatočnosti, podporuje sa mukociliárny klírens spúta, zvyšuje svalová masa a svalová sila.
Je jednoznačne potvrdená skutočnosť, že pravidelné denne kondičné cvičenie predlžuje život pacientov, ale zlepšuje aj kvalitu života a funkčné parametre pľúc.
Lieky
Bronchodilatačné lieky zlepšujú pľúcne funkcie u pacientov s CF a môžu znižovať frekvenciu ATB liečby. Dôležitý význam má tiež ich podávanie pred fyzioterapiou, zlepšujú mukociliárny klírens dýchacích ciest.
Mukolytiká sú dôležitou skupinou liekov, ktoré uľahčujú očisťovanie dýchacích ciest od hustého viskózneho hlienu. Jedným z prelomových mukolytík je inhalačne aplikovaná rekombinantná ľudská DNAza (alfa dornáza – Pulmozyme). Ďalším účinným mukolytikom je hypertonický roztok NaCl, N-acetylcystein (Solmucol, ACC) a najnovšie inhalačný manitol (Bronchitol).
Imunomodulátory a protizápalové lieky majú veľký význam pri potláčaní chronického zápalu, ktorý je najzávažnejším dôvodom deštrukcie dýchacích ciest pri CF. Túto skupinu liekov predstavujú napr. makrolidy, kortikosteroidy, nesteroidné antiflogistiká (ibuprofén). Ich nevýhodou je, že dlhodobé užívanie môže niesť riziko nežiadúcich účinkov.
Antibiotiká sú neodmysliteľnou súčasťou liečby CF a spôsob ich podania závisí od kultivačne zistenej baktérie a výber sa riadi citlivosťou na antibiotiká, alebo potvrdeným synergickým účinkom zvolených antibiotík.
Oxygenoterapia – liečba kyslíkom môže byť podávaná pacientom dočasne pri zhoršení stavu, alebo pri poklese saturácie artériovej krvi. Ak nedôjde k normalizácii saturácie mal by byť pacient nastavený na dlhodobú domácu oxygenoterapiu v trvaní aspoň 16 hodín denne.
Transplantácia pľúc je posledná možnosť riešenia závažného pľúcneho poškodenia pri CF. K transplantácii je pacient indikovaný ak splní určité kritéria, ku ktorým patrí napr. pokles FEV1 pod 30%, masívne hemoptýzy, rýchla progresia respiračnej insuficiencie, zvýšená frekvencia hospitalizácii, prekročenie stanovených hodnôt O2 a CO2. Dôležitým predpokladom úspešnej transplantácie a potransplantačného priebehu je dobrá fyzická kondícia pacienta.
Nádejou do budúcnosti pri liečbe CF je génová terapia, na ktorej pracujú vedci-odborníci a hľadajú spôsoby prenosu opraveného génu CFTR do bunky. To by malo pacientov zbaviť choroby a jej príznakov.
Ochorenie je liečiteľné, ale nie vyliečiteľné. Atypické formy môžu byt monosymptomatické (iba čiastočne vyjadrené). Terapia je symptomatická a nutná je častá liečba komplikácii. Prognóza sa s modernou liečbou zlepšuje, avšak 35 rokov sa dožije len 50% chorých. Deti sú sledované v centrách pre CF. Spravidla sú hospitalizované 3x ročne pre potrebu preliečenia antibiotikami. Akékoľvek infekcie sú riešené v centrách pre CF.
Tráviaci trakt: Nutný je dostatočný prívod živín - o 20 - 40 % viac ako u ostatných rovesníkov. Pre nedostatok tráviacich enzýmov je potrebné podávať enzýmy v tabletovej forme.
- Chronické sinopulmonálne ochorenia
- trvalé kolonizácie alebo infekcie dolných ciest dýchacích patogénmi typickými pre CF: S. aureus, H. influenzae, P. aeruginosa a B. cepacia
- chronický kašeľ a produkcia hlienu
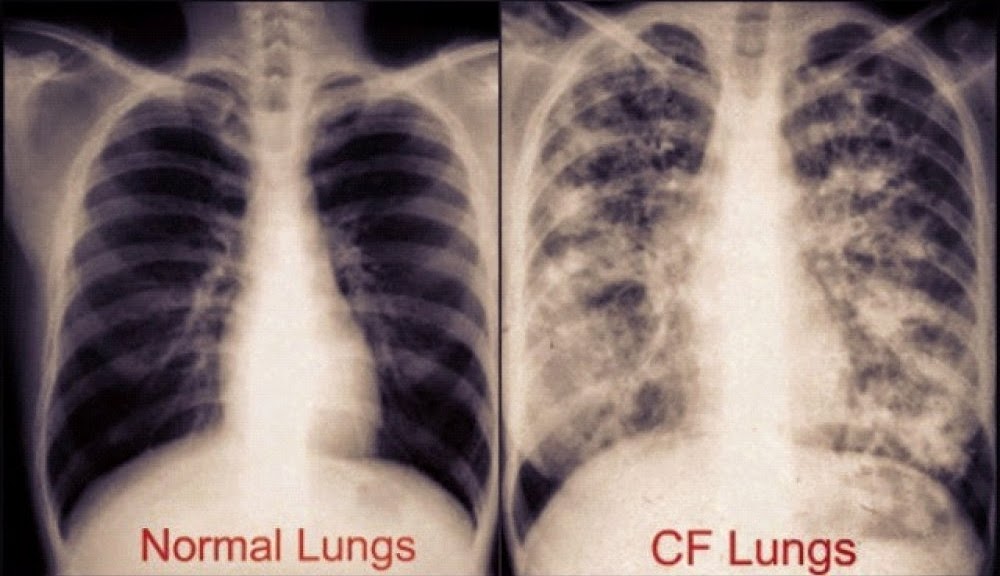
- charakteristické RTG zmeny (bronchiektázie, atelektázy, infiltráty…)
- obštrukcia dýchacích ciest pri funkčnom vyšetrení pľúc
- nosové polypy, radiologické alebo CT abnormality prínosových dutín
- paličkové prsty
- progresia obštrukčnej ventilačnej poruchy pľúc, rozvoj pľúcnej hypertenzie a chronického pľúcneho srdca
- Gastrointestinálne ochorenia
- intestinálne (choroby čreva) – mekóniový ileus, prolaps rekta, DIOS
- pankreatické – pankreatická insuficiencia, rekurentná pankreatitída,
- hepatálne – chronické hepatálne ochorenie (biliárna alebo multilobulárna cirhóza)
- Nutričné abnormality
- neprospievanie (proteínová a kalorická malnutrícia),
- sekundárna deficiencia v tukoch rozpustných vitamínov,
- hypoproteinémia a edémy
- Syndróm straty soli
- akútna deplácia soli
- chronická metabolická alkalóza
- Obštrukčná azoospermia – mužská urogenitálna abnormalita
Pre spojenie sa s ďalšími ľuďmi s rovnakou diagnózou vo vašom okolí sa prihláste.
Prihlásenie